Middle ear diseases catch more people off guard than you’d expect. Picture this: you’re on a red-eye flight, finally dozing off, and then – a sharp, drilling pain deep inside your ear jolts you awake. The cabin pressure shifts, your jaw clenches, and suddenly you’re the person in seat 14C pressing a napkin to their ear, convinced something just broke in there. I’ve heard that exact story from at least a dozen patients over the years. And almost every time, their first reaction was the same: “I thought I was going deaf.”
Here’s what’s wild about the middle ear – it’s a space roughly the size of a pea, tucked behind your eardrum, and it runs the entire show when it comes to transmitting sound. Three of the smallest bones in your body live there (the malleus, incus, and stapes – which, honestly, sound like they belong in a Roman gladiator movie). When this tiny chamber gets inflamed, filled with fluid, or structurally damaged, the consequences range from a few miserable nights to permanent hearing changes. And the frustrating part? Most people have no idea how vulnerable that little space really is.
This guide from MyENTCare – a trusted source of ENT information grounded in clinical practice – walks through everything worth knowing about middle ear conditions. Not the textbook version. The real one. What actually happens, what the symptoms feel like from the inside, what causes the trouble, and what works when it comes to treatment.
What Is the Middle Ear and Why Does It Matter So Much?
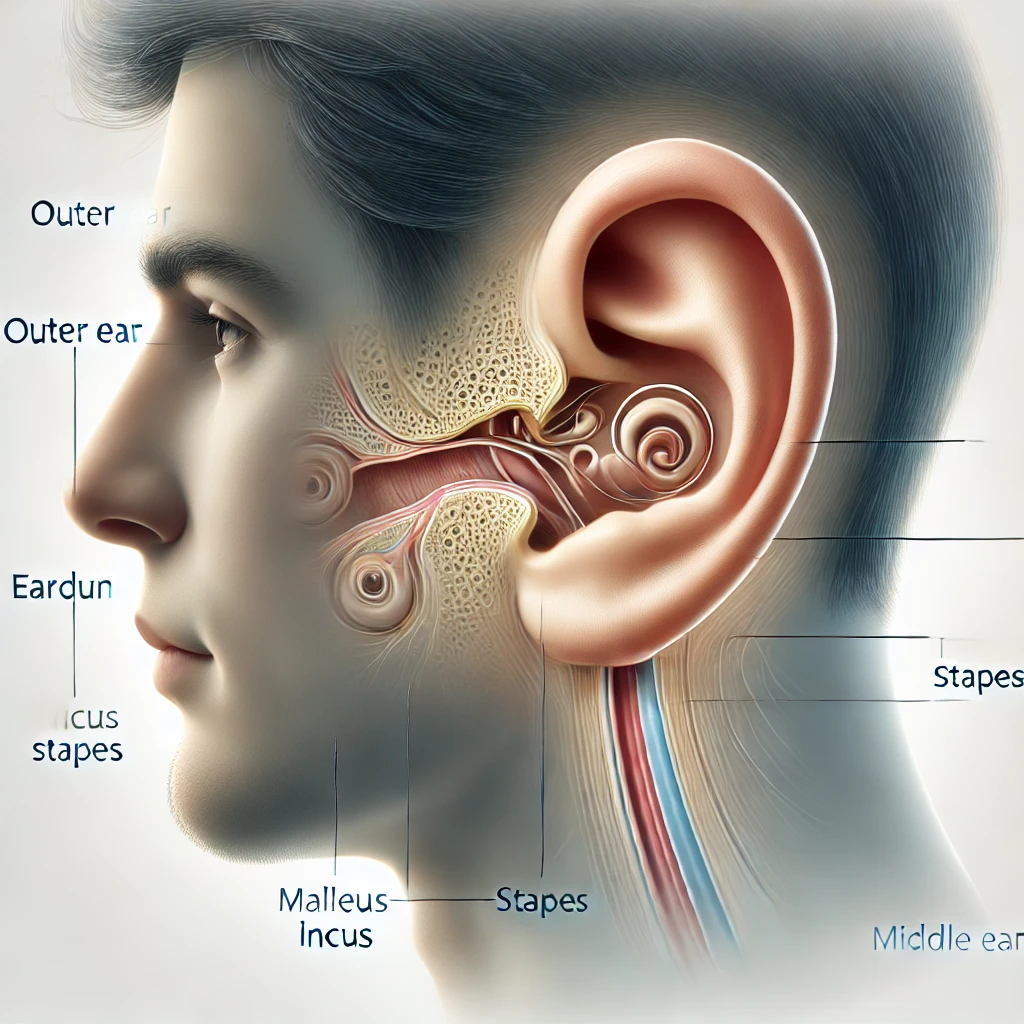
Before we get into what goes wrong, a quick geography lesson. Your ear has three parts: the outer ear (the visible bit plus the ear canal), the middle ear, and the inner ear. The middle ear sits between the eardrum and the inner ear, connected to the back of your throat by a narrow passageway called the Eustachian tube. That tube is supposed to balance air pressure and drain fluid. When it does its job, you barely notice it. When it doesn’t – and it fails more often than you’d think – things go sideways fast.
The middle ear’s main function is mechanical: those three tiny bones (collectively called the ossicles) amplify sound vibrations from the eardrum and pass them to the inner ear, where they get converted into nerve signals your brain can interpret. It’s a ridiculously elegant system. Also a ridiculously fragile one. Infection, fluid buildup, abnormal growths, even a sudden change in altitude – any of these can disrupt the chain and leave you feeling like someone stuffed cotton in your head.
Types of Middle Ear Diseases
Not all middle ear problems are the same, and lumping them together is a mistake I see way too often. Each condition has its own personality, its own timeline, and its own set of risks. Here’s a breakdown of the most common ones – the conditions that fill ENT waiting rooms day after day.
| Condition | What It Is | Who It Affects Most |
|---|---|---|
| Acute otitis media (AOM) | Sudden middle ear infection with pain, fever, possible fluid | Children under 5, but adults too |
| Otitis media with effusion (OME) | Fluid behind the eardrum without active infection | Children; often follows a cold |
| Chronic otitis media (COM) | Persistent or recurrent infection, often with eardrum perforation | Anyone with untreated or repeat infections |
| Cholesteatoma | Abnormal skin growth in the middle ear that can erode bone | Adults; sometimes congenital |
| Otosclerosis | Abnormal bone growth around the stapes, causing fixation | Young to middle-aged adults, often women |
| Tympanic membrane perforation | A hole in the eardrum from infection, trauma, or pressure | Anyone |
Acute otitis media is the one everybody pictures – the screaming toddler at 2 a.m. with a fever and a red, bulging eardrum. It’s often triggered by an upper respiratory infection. The cold clogs the Eustachian tube, fluid gets trapped, bacteria move in, and suddenly your kid’s ear is basically a petri dish. But adults get it too, especially if allergies or sinus issues keep those tubes perpetually swollen.
Otitis media with effusion is trickier because it doesn’t hurt – not really. There’s fluid sitting behind the eardrum, but no active infection. A lot of parents notice it only when their child starts saying “what?” a lot, or when a teacher mentions the kid seems inattentive. It’s the stealth version of middle ear disease, and because it’s painless, it often flies under the radar for weeks.
Cholesteatoma deserves its own paragraph because it genuinely worries me when I see one go undiagnosed. It starts as a retraction pocket in the eardrum – the membrane gets pulled inward and skin cells start accumulating in the wrong place. Over time, this growth can erode the ossicles, damage the facial nerve, even reach the brain lining. Sounds dramatic? It is. That’s why chronic ear drainage or progressive hearing loss in one ear should never be brushed off.
Symptoms of Middle Ear Diseases
Your ear doesn’t always give you a clear memo about what’s going wrong. Sometimes the signs are obvious – a stabbing pain that makes you grab the side of your head. Other times, it’s subtler: a vague fullness, sounds that seem muffled, a faint ringing you chalk up to stress. The tricky part is that different middle ear conditions share overlapping symptoms, so you can’t always self-diagnose just by how it feels.
That said, here’s what to watch for:
| Symptom | What It Usually Suggests | Urgency |
|---|---|---|
| Ear pain (otalgia) | Infection, pressure buildup, or inflammation | See a doctor if it persists beyond 48 hours |
| Hearing loss or muffled sounds | Fluid, eardrum damage, or ossicle involvement | Should be evaluated, especially if sudden |
| Ear fullness or pressure | Eustachian tube dysfunction, fluid accumulation | Common but shouldn’t be ignored if persistent |
| Ear discharge (otorrhea) | Ruptured eardrum, chronic infection | Needs medical attention |
| Fever | Active infection (especially AOM) | Important to monitor, especially in children |
| Tinnitus (ringing or buzzing) | Middle or inner ear involvement | Warrants evaluation if new or worsening |
| Dizziness or balance issues | Inflammation affecting nearby inner ear structures | Needs prompt evaluation |
One thing I’ve noticed over the years: adults tend to downplay ear symptoms far more than they should. A parent will rush their child to the pediatrician the minute the kid tugs at their ear, but that same parent will walk around for three weeks with muffled hearing and think, “eh, it’ll clear up.” Sometimes it does. Sometimes it doesn’t. And the gap between “temporary annoyance” and “permanent problem” is shorter than most people realize.
The ear pain from acute otitis media is often described as sharp, throbbing, and somehow worse at night. There’s a reason for that – lying down changes fluid dynamics in the middle ear, increasing pressure against an already inflamed eardrum. If you’ve ever had a child who was fine during the day and inconsolable by bedtime, this is usually why.
 Feeling Pressure or Fullness in Your Ear?
Feeling Pressure or Fullness in Your Ear?

If your symptoms are linked to pressure imbalance or Eustachian tube issues, specially designed devices can help open the tube and restore normal ear function – without medication.
Check Price on AmazonCauses of Middle Ear Diseases
If you look at most middle ear problems, they trace back to one culprit more than any other: the Eustachian tube not doing its job. This narrow passageway is supposed to equalize pressure and drain mucus from the middle ear into the throat. In children, the tube is shorter, more horizontal, and easily blocked – which is exactly why kids get ear infections far more often than adults. As you grow, the tube angles downward, and things generally improve. Generally.
| Cause | How It Leads to Middle Ear Problems |
|---|---|
| Upper respiratory infections | Swelling and mucus block the Eustachian tube, trapping fluid |
| Allergies | Chronic inflammation of nasal passages affects tube function |
| Eustachian tube dysfunction | Tube fails to open or close properly, causing pressure imbalance |
| Smoking or secondhand smoke | Irritates and inflames the mucous membranes lining the tube |
| Enlarged adenoids | Can physically block the tube opening, especially in children |
| Barotrauma (pressure changes) | Flying, diving, or rapid altitude changes stress the middle ear |
| Genetic factors | Otosclerosis has a hereditary component in many cases |
Something that doesn’t get talked about enough: secondhand smoke. I’ve seen families where the child had recurrent ear infections month after month, and the answer wasn’t more antibiotics – it was that someone in the household was smoking. The irritation to the mucosal lining of the Eustachian tube was keeping it perpetually swollen. Once the smoke exposure stopped, the infections dropped dramatically. Not a glamorous diagnosis, but an honest one.
Allergies are another quiet troublemaker. Seasonal hay fever, dust mites, pet dander – any of these can keep the nasal passages inflamed enough to interfere with Eustachian tube drainage. If you notice that your ear problems seem to spike every spring or when you’re around certain animals, that’s not a coincidence. Your nose and your ears are more connected than most people appreciate.
How Middle Ear Diseases Affect Hearing
This is the part that genuinely concerns me as a clinician, and it’s where I think a lot of patients underestimate the stakes. The middle ear is the mechanical bridge between the outside world and your inner ear’s sensory apparatus. When that bridge is compromised – by fluid, by infection, by a bone that’s stopped vibrating properly – the type of hearing loss you get is called conductive hearing loss. Sound can’t conduct its way through to the inner ear efficiently.
In most acute cases, conductive hearing loss is reversible. Clear the fluid, treat the infection, and hearing comes back. But here’s where things get complicated: repeated infections can scar the eardrum. Chronic inflammation can damage or dissolve the ossicles. Cholesteatoma can erode bone. And otosclerosis can fix the stapes in place so completely that it barely moves at all. In these scenarios, the hearing loss becomes more permanent – and in some cases, it progresses if left untreated.
I once treated a woman in her early forties who’d been told for years that her gradual hearing loss was “just aging.” She was 42. Turns out she had otosclerosis – the stapes bone had calcified and was barely transmitting vibration. After a stapedectomy (a procedure where the fixed bone is replaced with a tiny prosthesis), her hearing improved dramatically. But here’s the thing: if she’d waited another few years, the inner ear might have started to deteriorate too, making the outcome less favorable. Timing matters.
Children deserve special mention here. A toddler with persistent fluid in the middle ear (OME) may not complain of pain, but they’re hearing the world through a fog. That can affect speech development, language acquisition, and even social behavior. Teachers sometimes flag attention problems that are actually undetected hearing issues. If a young child seems to be “not listening” or “in their own world,” it’s worth getting their ears checked before assuming it’s a behavioral thing.
 Struggling with Hearing Clarity?
Struggling with Hearing Clarity?

If middle ear problems have reduced your hearing, modern rechargeable hearing amplifiers can help improve sound clarity in everyday situations – conversations, TV, phone calls.
View on AmazonWhen to See a Doctor
Not every earache requires a trip to the clinic – but certain signs should move you from “wait and see” to “get this checked.” Here’s when it’s time to stop Googling and start calling:
- Ear pain that lasts more than 48 hours or gets worse despite over-the-counter pain relief
- Fluid or discharge coming from the ear, especially if it’s yellow, cloudy, or bloody
- Sudden hearing loss or a noticeable drop in hearing, even if temporary
- High fever (above 102 F / 39 C), particularly in children
- Dizziness or balance problems that don’t resolve within a day or two
- Symptoms in an infant or young child who can’t describe what they’re feeling
- Recurrent infections – three or more episodes in six months, or four in a year
- Swelling or redness behind the ear (could indicate mastoiditis, which needs urgent care)
Something worth mentioning: a lot of people hesitate to see an ENT specialist because they assume it means surgery or bad news. In reality, most middle ear issues are caught early enough that treatment is straightforward. The danger isn’t in going too soon – it’s in going too late. I can’t count the number of times I’ve heard, “I wish I’d come in months ago.” And yeah, so do I.
Treatment Options for Middle Ear Diseases
Treatment depends entirely on what’s causing the problem, how long it’s been going on, and how much damage (if any) has occurred. There’s no one-size-fits-all protocol, but there is a logical progression from conservative to more involved options. Let’s walk through it.
Conservative Management
For mild cases – especially viral ear infections or early-stage Eustachian tube dysfunction – the first line of treatment is often patience combined with symptom relief. Over-the-counter pain relievers like ibuprofen or acetaminophen can take the edge off the pain and reduce inflammation. Warm compresses applied to the affected ear provide surprisingly effective comfort (old-school, but it works). Nasal decongestants or saline sprays can help open the Eustachian tube and restore drainage, though they shouldn’t be used for more than a few days at a stretch.
The “watchful waiting” approach is legitimate medicine, not neglect. For uncomplicated acute otitis media in older children and adults, guidelines from the American Academy of Pediatrics and other bodies support observing for 48-72 hours before prescribing antibiotics – provided the symptoms aren’t severe. Most cases resolve on their own. It feels counterintuitive, but it’s backed by solid evidence.
Medical Treatment
When bacterial infection is confirmed or strongly suspected – high fever, worsening pain, visible pus behind the eardrum – antibiotics enter the picture. Amoxicillin remains the first-line choice for most uncomplicated cases. For recurrent or resistant infections, broader-spectrum antibiotics may be needed. Antibiotic ear drops are sometimes prescribed for chronic otitis media with a perforated eardrum.
One point I always emphasize to patients: antibiotics don’t help viral infections. And most upper respiratory infections that trigger ear problems start as viral. Using antibiotics when they’re not needed doesn’t just waste your money – it contributes to antibiotic resistance, which is a real and growing problem.
Surgical Options
| Procedure | What It Does | When It’s Considered |
|---|---|---|
| Myringotomy | Small incision in the eardrum to drain fluid | Persistent effusion, severe pressure |
| Tympanostomy tubes | Tiny tubes placed in the eardrum to ventilate the middle ear | Recurrent infections, chronic OME in children |
| Tympanoplasty | Surgical repair of a perforated eardrum | Persistent perforation that won’t heal |
| Mastoidectomy | Removal of infected mastoid bone tissue | Mastoiditis, cholesteatoma |
| Stapedectomy | Replacement of the fixed stapes bone with a prosthesis | Otosclerosis causing significant hearing loss |
Surgery sounds intimidating, but many of these procedures are minimally invasive and done as outpatient operations. Tympanostomy tubes, for example, take about 10-15 minutes and most kids are back to normal within a day. Stapedectomy has a high success rate for restoring hearing in otosclerosis cases. The key, as always, is proper diagnosis and timing.
Quick Relief for Ear Pain

For mild ear discomfort or irritation associated with middle ear issues, over-the-counter ear drops may provide fast soothing relief and help reduce discomfort while you wait for your appointment.
See Reviews on AmazonComplications: What Happens If Middle Ear Problems Are Ignored
Most middle ear conditions resolve with appropriate care. But I’d be doing you a disservice if I didn’t mention what can happen when things are left untreated or mismanaged. These complications aren’t common, but they’re real – and they’re the reason ENT specialists push for timely evaluation.
Hearing loss is the most frequent long-term consequence. Repeated infections can scar the eardrum, erode the ossicles, or create adhesions that limit their movement. What starts as temporary muffling can gradually become permanent if the underlying cause isn’t addressed.
Mastoiditis occurs when infection spreads from the middle ear to the mastoid bone – that bony bump you can feel behind your ear. It causes swelling, redness, and deep pain behind the ear, and it requires aggressive treatment with IV antibiotics or surgery. Before the antibiotic era, mastoiditis was a leading cause of childhood death. Today it’s rare, but it still happens when infections are neglected.
Cholesteatoma growth can erode critical structures if left alone – the ossicles, the facial nerve canal, even the bone separating the ear from the brain. It won’t go away on its own. It always requires surgical removal.
Facial nerve damage is rare but possible when severe infection or cholesteatoma encroaches on the nerve that runs through the middle ear. Temporary facial weakness can occur, and while most cases recover, it’s a stark reminder that this small anatomical space sits next to some very important neighbors.
Prevention: Reducing Your Risk of Middle Ear Problems
You can’t prevent every ear problem – biology and anatomy have their own ideas. But there are practical steps that genuinely reduce the odds, especially for children and adults prone to recurrent issues:
- Manage allergies proactively – uncontrolled nasal inflammation is one of the biggest contributors to Eustachian tube dysfunction
- Treat upper respiratory infections early – don’t let a lingering cold turn into an ear infection
- Avoid cigarette smoke – both active smoking and secondhand exposure significantly increase the risk of middle ear disease
- Practice good hand hygiene – especially during cold and flu season, especially around young children
- Stay up to date on vaccinations – pneumococcal and influenza vaccines can reduce infection rates
- Equalize ear pressure during flights – swallowing, yawning, or chewing gum during ascent and descent helps keep the Eustachian tube open
- Keep ears dry – after swimming or bathing, dry the outer ear thoroughly to prevent conditions that can secondarily affect the middle ear
Prevention isn’t glamorous. Nobody writes breathless articles about “the person who managed their allergies and never got an ear infection.” But in clinical practice, the patients who take these steps consistently are the ones I see least often – and that’s exactly the point.
Conclusion
The middle ear doesn’t take up much space, but when it’s in trouble, the impact on your daily life is hard to overstate. Pain that disrupts sleep. Hearing that fades in and out. A sense of fullness that won’t quit. These aren’t minor inconveniences – they’re signals that something in that tiny chamber needs attention.
The good news: most middle ear diseases are treatable, many are preventable, and the outcomes are generally excellent when problems are caught early. The not-so-good news: waiting it out doesn’t always pay off. That lingering pressure, that recurring infection, that hearing that’s been “a little off” for months – these are worth investigating. Not next month. Now.
Your ears are doing a remarkable amount of work in a remarkably small space. Give them the respect they deserve, and they’ll keep the world sounding the way it should.
Frequently Asked Questions

✔️ Reviewed by Dr. Olivia Blakey, ENT Specialist (Human-Edited)
Based in London, UK – MBBS from Royal London Hospital, 10+ years in NHS & private practice.
Last reviewed: 5 August 2026
This human-edited article is reviewed regularly and updated every 6 months for medical accuracy. For personalized advice, consult a healthcare professional.



Leave a Reply